
Research Article | DOI: https://doi.org/10.31579/2768-0487/020
*Corresponding Author: Onwurah O.W, Department of Haematology, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria.
Citation: Onwurah O.W, Ajuba C.I, Nwoke C.G, Anokwute M.U, Nkemjika U.N, et al (2021) Prevalence of Hepatitis B e-Antigen among Hepatitis B positive subjects in Nnamdi Azikiwe University Teaching Hospital Nnewi. Journal of Clinical and Laboratory Research. 3(1) DOI:10.31579/2768-0487/020
Copyright: ©2021 Onwurah O.W. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 April 2021 | Accepted: 29 April 2021 | Published: 11 June 2021
Keywords: prevalence; HBeAg; NAUTH; Nnewi
Hepatitis B virus (HBV) is a common cause of liver disease throughout the world. Cirrhosis, liver failure and hepatocellular carcinoma develop in 15–40% of chronically infected hepatitis B virus individuals. HBV is transmitted through blood and other body fluids, including semen and saliva. The aim of this study was to determine the prevalence of HBeAg amongst HBsAg positive subjects in Nnamdi Azikiwe University Teaching Hospital, Nnewi (NAUTH) . This study was a cross sectional study and data were collected through oral interview and questionnaire. Five milliliters of blood was collected aseptically from the antecubital veins of consenting 100 HBsAg positive subjects into sterile containers free of anticoagulants. The sample was separated by low- speed centrifugation and the serum obtained was analyzed for HBsAg and HBeAg using diagnostic HBsAg panel kit (Diagnostic Automation/ Cortez Diagnostic Inc, USA). The result showed 6% HBeAg prevalence among the 100 HBsAg-positive patients in NAUTH. The HBsAg patients that tested positive for HBeAg were all males. The study concluded low prevalence of HBeAg among HBsAg patients in NAUTH.
Hepatitis B virus (HBV) is a common cause of liver disease throughout the world. Cirrhosis, liver failure and hepatocellular carcinoma develop in 15–40% of chronically infected hepatitis B virus individuals [1]. HBV is transmitted through blood and other body fluids, including semen and saliva. The virus is hundred times more infectious than human immunodeficiency virus (HIV) and unlike HIV; it can live outside the body in dried blood for longer than a week [2]. It may present as acute hepatitis with resolution or chronic hepatitis which may evolve to cirrhosis and fulminant hepatitis with massive liver necrosis and the backdrop for hepatitis D virus infection.
Chronic HBV infection is defined as hepatitis B surface antigen (HBsAg) positivity for at least six months [3]. Over 350million of the 2 billion individuals infected with hepatitis B virus worldwide are chronically infected [4]. An estimated one third of the world’s population has serologic HBV infection occurs frequently in Nigeria [5]. It is estimated that about 12% of the total Nigerian population of 140 million is chronically infected with Hepatitis B virus [6]. The global prevalence of chronic hepatitis B infection varies widely, from >8% in Africa, Asia, and the Western Pacific to 2–7% in Southern and Eastern Europe, and to <2% in Western Europe, North America, and Australia. In the United States of America, an estimated 185,000 new infections evolved yearly [7]. In Nigeria, hepatitis B virus (HBV) infection has reached hyper-endemic levels [8]. HBV is a DNA virus that replicates asymmetrically via a reverse transcription of an RNA intermediate, making it prone to mutations in the genome at an approximate rate of one nucleotide/10,000 bases/infection year [9].
Hepatitis B e -antigen (HBeAg) is derived from the translation product of the precore and core regions. It is selected from the infected hepatocyte because of a secretory signal sequence at the beginning of the precore region [10]. Seroconversion from HBeAg to e antibody (anti-HBe) is usually accompanied with cessation of HBV replication, remission of liver disease with a decrease in serum HBV viral load and is associated with a favourable prognosis [1].
There are eight major genotypes of HBV, and these have been shown to have distinct geographical preference [11]. HBV genotype E is almost restricted to West Africa, including Nigeria where this genotype is predominant [12].
The expression of HBeAg may vary depending on the genotype just as clinical outcome and response to antiviral treatment in different population groups have been associated with varying viral genotypes [13]. Several studies have shown that HBeAg is a biomarker of active viral proliferation in hepatocytes, infectivity, and transmission and is associated with an increased risk of hepatocellular carcinoma [14].
A cross-sectional study of the Prevalence of HBeAg among hepatitis B positive subjects in NAUTH was carried out. A total of 100 HBsAg-positive subjects were used. Five milliliters (5mls) of blood specimen was collected by aseptic technique from the antecubital veins of each consenting HBsAg positive subjects into sterile containers free of anticoagulants or preservatives. Serum samples were separated and aseptically transferred into labeled sterile tubes and the analysis carried out within one hour of sample collection. Diagnostic panel kit for HBV infection marker (Diagnostic Automation/ Cortez Diagnostic Inc, USA) Technique was used. The reactions were observed and result recorded within 15 minutes. Statistical package for social science (SPSS) version 23 was used for data analysis: simple prevalence, chi-square analysis was used where necessary and level of significance will be set at 95% confidence interval at (0.05 and 0.01). Risk factors were assessed using association (chi-square analysis).
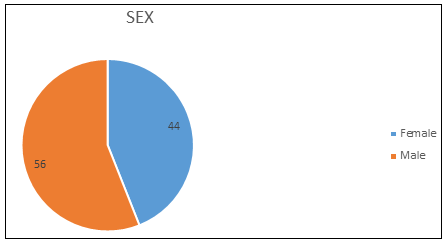
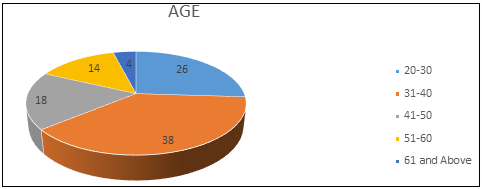
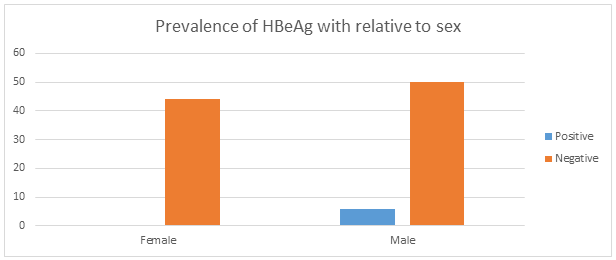
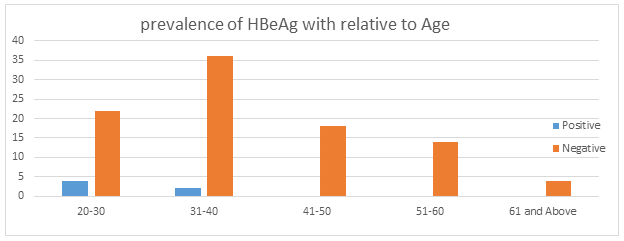
A total of 100 HBsAg-positive subjects were screened for the prevalence of HBeAg in NAUTH. Males were 56 in number while the females were 44; all were HBsAg-positive subjects (Figure 1). Their ages ranged from 20 to 63 years (Figure 2). Six (6.0%), were found to be positive for HBeAg and 94 (94.0%) were negative. The 6% positive for HBeAg were all male. X2 (chi-square) was used to test the significant difference in the association between sex and prevalence of HBeAg and the result showed that there exists a significant difference in the association between sex and prevalence of HBeAg with X2 = 5.015, df = 1 and p-value = 0.025which is less than 0.05 (Figure 3). Figure 4 shows that the 6 patients tested positive for HBeAg, 4 (66.7%) were between ages 20-30 whereas 2 (33.3%) were between ages 31-40. X2 (chi-square) was used to test the significant difference in the association between age and prevalence of HBeAg and the result showed that there exists no significant difference in the association between age and prevalence of HBeAg with X2= 6.394, df = 4 and p-value = 0.172 which is greater than 0.05
Hepatitis B Virus (HBV) is classified into eight genotypes (designated by letters A-H) on the basis of divergence of 8% or more in the nucleotide sequence, and they have distinct geographical distributions [11]. The expression of HBeAg may vary depending on the genotype just as clinical outcome and response to antiviral treatment in different population groups have been associated with varying genotypes [13]. The problem of HBV infection in Nigeria is well-recognized, especially among virologists and hepatologists but efforts to control the virus have not been satisfactory as a significant impact on disease incidence or prevalence has not been observed. The presence of HBeAg in the serum of subjects with hepatitis B virus is a reflection of active viral replication in hepatocytes and is considered a surrogate marker for the presence of the DNA of hepatitis B virus [15]. Testing for the HBeAg can also identify individuals with a high risk of developing liver cancer [14].
In this study, 6% HBeAg prevalence was recorded among HBsAg-positive subjects in Nnamdi Azikiwe University Teaching Hospital, Nnewi (NAUTH) Nigeria. This reflects a pool of individuals who are highly infectious and serve in sustaining viral transmission and evolution in the Nigerian population, suggesting that the future burden of liver cancer associated with HBV is likely to be high. Other previous studies, in Enugu [16], low prevalence at 8.6% was found among asymptomatic adults. In Benin City, the overall HBe-antigenaemia prevalence among adults was 7.3% [17]. Among blood donors in Ibadan [18], 4 of 37 HBsAg (10.8%) were HBeAg-positive. Patients with a clinical, ultrasound and/or histological evidence of liver cirrhosis or HCC in Lagos [19] and prisoners in south-eastern Nigeria [20], both areas showed that HBeAg was present respectively in 11.9% and 16.4% HBsAg-positive individuals. From these studies, it appears that there is a marked geographical difference in the prevalence of HBeAg among HBsAg-positive subjects in Nigeria, with northern Nigeria showing a higher prevalence when compared with the southern Nigeria. This, however, seems not to be the case. In Ile-Ife [21] and in Ibadan [22], report showed 48.4% and 19% HBeAg seropositivity respectively among HBsAg-positive patients in Nigeria. Taken collectively and following documented evidence in Nigeria, it is clear that high infectivity of the virus is widespread among Nigerians with HBV infection [22], and knowing full well that HBeAg is associated with active liver disease [17]. It is, therefore, important that healthcare facilities in Nigeria should attempt to implement routine HbeAg testing of blood of all HBV-positive patients to determine the status of infection and to adequately plan for proper patient management.
In this study, 6% of all HBeAg-positive individuals were males. There seem to be preponderance for males to have active HBV infections. This correlates with studies (from Enugu and Benin City, Nigeria), which found that the number of HBeAg-positive males were more than double the number of females [16]. So, it remains to be determined whether the gender differences observed in this study is the true reflection of the gender distribution or is associated with the study population or the healthcare-seeking patterns of Nigerians in this region. This research showed that there is a significant difference in the association between age and prevalence of HBeAg among the subjects studied, this is in line with what was reported by [23], which revealed that the prevalence of HBeAg was higher in subjects between the age group of 10-20 years and appeared to decrease with increase in age.
This research has shown that 6.0% of HbsAg-positive individuals studied were also positive for HbeAg, which is a marker of active viral replication and transmission. This is also taken as an indication of active HBV in the Nigerian population, and is unacceptable despite the effective vaccine which has been available since 1982.
Strengthening of the childhood vaccination programme, massive intervention activities, and treatment programmes to reverse the possible devastating effect of HBV infection is highly recommended which will go a long way in reducing the transmission of HBV. The success of these efforts will depend on our resolution to make the elimination of HBV infection a top priority on the public-health agenda in Nigeria.
Authors have declared that no competing interests exist.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
